This is long but I thought I would share for those that are interested in learning about Breast cancer and reconstruction ( at least the kind I had)
Breast Cancer Reconstruction History
Documented cases of breast cancer date back to 6000 BC, andfollowing its history over the centuries is harrowing to say the least. IfCleopatra had breast cancer, the ancient Egyptian doctors would have cauterizedher breast in hopes of burning out the disease. The treatment was so untenablethat women neglected their disease if a lump was discovered. Their breastsbecame disfigured as their tumors took over their bodies. But the alternativewas worse than the disease. George Washington’s mother succumbed to breastcancer. So did Queen Mary. Nabby Adams, the daughter of John and Abigail Adams,suffered through a mastectomy in which she was tied to a chair and withoutanesthesia her breast was removed. She survived the surgery only to die fromthe disease. This was common practice in the 18th century.
In the 19th century, anesthesia was developed and surgicaloptions improved a great deal. Breast cancer surgery was revolutionized by Dr.William Halsted, who popularized the radical mastectomy as the treatment ofchoice for any woman with breast cancer. Even though an extreme amount oftissue was removed, women were surviving the operation and their breastcancers. He removed not only the breast, but the lymph nodes and the chestmuscles. In some extreme cases, other surgeons performing radical mastectomiesincluded removing part of the rib cage. This was so disfiguring though that thepractice was soon stopped.
It was not until the latter half of the 20th century and theawakening of the women’s movement that these radical procedures werequestioned. Modified radical mastectomy (total mastectomy with axillary lymphnode dissection) was perfected. Breast conservation therapy consisting oflumpectomy, sentinel lymph node biopsy and radiation was developed. The emergenceof breast cancer reconstruction took off.
The Evolution ofBreast Implants
During World War II, Dow Chemical Company created commercialuses for silicone. The first use of silicone breast implants for cosmeticbreast augmentation occurred in 1962. Dow Corning, along with several othercompanies, started manufacturing implants both for cosmetic augmentation andreconstruction after mastectomies. Women found that silicone implants lookedand felt better than the saline alternative.
However, those early generation devices exhibited problems overtime. Silicone leakage led to breast scarring and sometimes painfuldeformities. Allegations that breast implants could cause cancer or autoimmunediseases were made by health care advocacy groups, fueling mass litigation. Bythen over one million women had silicone implants. In 1992, the Food and DrugAdministration banned them. David Kessler, the head of the FDA stated, “We wantsurgeons to stop using these implants in patients until this new evidence canbe thoroughly evaluated, I’m asking patients to understand that the Food andDrug Administration commissioner cannot assure the safety of these devices atthe present time.” Dow Corning stopped producing implants and later went intoChapter 11 bankruptcy.
Between 1992 and 2006 saline filled breast implants remainedthe only fully-approved type of implant on the market in the United States.Patient satisfaction was, and remains good, but the interest in siliconeimplants continued. During this period large scale studies of the healtheffects of silicone implants were performed. Numerous reports from institutionsincluding the Mayo Clinic, the National Institute of Medicine, and otherindependent commissions all corroborated that there was no causal relationship betweenbreast implants and illnesses like cancer or lupus. This led to the nationaladjunct study which was commissioned to prospectively analyze the outcomes ofwomen using silicone implants for reconstruction. Plastic surgeons worked withthe two remaining U.S. implant manufacturers, Mentor and McGhan (nowInamed/Allergan) to report data in an FDA approved protocol.
Finally, in November of 2006, the Food and Drug Administrationreversed its ban on silicone-filled breast implants. The FDA’s press release stated, “The products havebeen determined to be safe and effective.” Now, silicone gel implants arewidely used for both cosmetic breast augmentation and breast cancerreconstruction. These newer generation silicone devices are the safest, softestand most natural implants to date. Both saline and silicone implants arepopular choices today.
The Evolution ofAutogenous Tissue Reconstruction
Numerous techniques have evolved to allow for breastreconstruction using natural tissues from a woman’s body rather than anartificial implant. The earliest techniques utilized muscles to provide bloodflow to skin and fat so that that this tissue could be transported to the chestto create a breast mound. The latissimus dorsi flap was the most popular formof autogenous tissue breast cancer reconstruction in the 1970s. Skin, fat andmuscle from the back were rotated to the front of the body to create a breast.Today, this procedure is used in conjunction with implants to provide a fullerlooking breast.
In 1982, the first TRAM flap (transverse rectus abdominus myocutaneous)procedure was performed. In this procedure, a woman’s lower abdominal skin andfat is used to make the breast. In this flap, the rectus abdominis muscle isused to support the skin and fat which is tunneled up into the breast area.Today, this flap remains the standard of care in this and other countries,creating natural appearing breasts and improved abdominal contours.
Nevertheless, there are drawbacks to using these muscles and sotechniques have evolved to minimize or eliminate the need for sacrificingmuscles for breast cancer reconstruction. The use of microvascular free flapsallows transplanting tissue from one part of the body to another without theuse of a large muscle. The abdomen is the source of many varieties of suchflaps. The TRAM free flap uses only a small portion of the rectus muscle, whilethe DIEP free flap (deepinferior epigastric perforator), and the SIEA free flap (superficial inferior epigastric)utilize none of the rectus muscle. The buttock is another source of skin andfat that can be used to create a breast. The GAP free flaps (gluteal artery perforator)allow a hidden donor site most useful for women with insufficient abdominaltissue. As a result of these procedures, women recover easier and have fewercomplications from the donor site.
All of these procedures, as well as the techniques for creatinga natural nipple and areola are explained further in the section on Types of Reconstruction.
The future is bright for breast reconstruction and breastcancer patients. It was a long, hard journey in the beginning. But with theadvent of systemic therapy, new surgical procedures, and a healthy partnershipbetween patient and doctor, women are living longer and looking better thanever before. This could be considered the golden age of breast cancerreconstruction. The only downside is trying to decide which procedure you want!
This is the type of reconstruction I had.
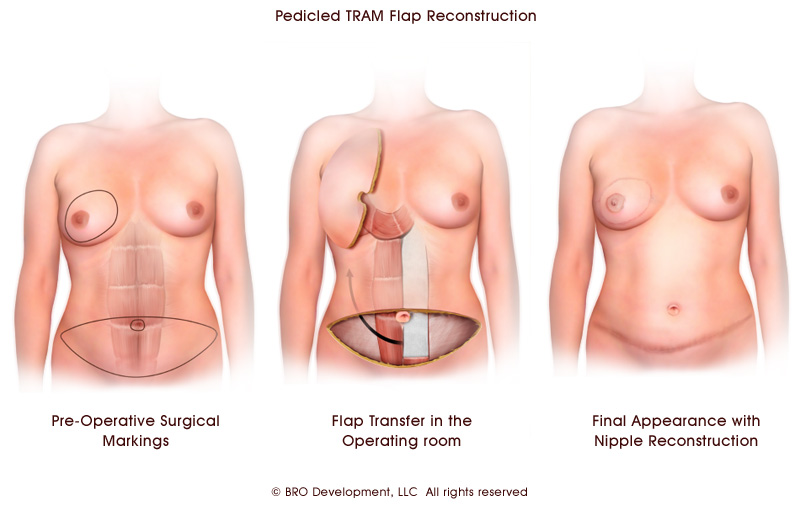
TRAM Flap
The most common method of autogeneous tissue reconstruction isthe pedicled transverse rectus abdominus myocutaneous (TRAM) flap. In thisapproach, the entire rectus abdominus muscle is used to carry the lowerabdominal skin and fat up to the chest wall. A breast shape is then createdusing this tissue. In order to transfer the flap to the chest, the muscle istunneled under the upper abdominal skin. Since the patient’s own body tissue isutilized, the result is a very natural breast reconstruction. Also, the patientwill have the benefit of a flatter looking abdomen. The scar on the abdomen islow, and extends from hip to hip. The TRAM flap can be used for reconstructingone or both breasts. In a patient undergoing unilateral reconstruction, theTRAM flap can potentially offer better symmetry than using an implant.
The TRAM flap is based on the superior epigastric vessels,which are considered to be the secondary blood supply to the lower abdominalwall skin. Some patients should not have this type of reconstruction because oflimitations in the flap blood supply. For example, smoking, diabetes, andobesity are considered to be relative contraindications to having a pedicledTRAM flap breast reconstruction.
While the benefit of the TRAM flap is a natural looking andfeeling breast, the primary disadvantages relate to the abdominal wall donorsite. These include potential abdominal wall weakness, bulging, and hernia. Toprevent hernia, most surgeons will use a synthetic mesh when closing theabdomen.
The TRAM flap operation is more involved than implantreconstruction. The length of surgery for a unilateral TRAM flap reconstructionis generally four to five hours. For bilateral reconstruction, it isapproximately five to seven hours. The hospital stay is usually three to fivedays. The patient will have abdominal pain and tightness for several weeks, andit can often several months to return to a full range of activity.
Secondary procedures after a TRAM flap reconstruction can bedone in about 3 months. However, if chemotherapy is needed, any additionalsurgery must await completion of treatment. At that point, the patient can haverevisions to the breasts and abdomen, and the nipple areola can be created.Such additional procedures are typically done as outpatient surgery with arapid recovery.
You are an ideal candidate for TRAM flap reconstruction if you:
- desire autogeneous reconstruction
- do not want or are not a candidate for implant reconstruction
- have enough lower abdominal wall tissue to create one or both breasts
- have not had prior abdominal surgery
- previously had chest wall radiation
- have had failed implant reconstruction
- are having immediate reconstruction at the time of skin-sparing mastectomy
- are having delayed reconstruction following prior mastectomy
You are not an ideal candidate for TRAM flap reconstruction ifyou:
- do not have enough lower abdominal tissue to create the flaps
- have a large overhanging pannus of abdominal skin and fat
- have a BMI of 30 or above
- have diabetes
- are a smoker or quit smoking only recently
- have had previous abdominal surgeries such as abdominoplasty
- cannot tolerate anesthesia for long periods
- do not wish to have a lower abdominal scar
NippleAreola Reconstruction
Creatingthe nipple areola is the final component to making your breast reconstructioncomplete. There have been numerous approaches to nipple reconstruction over thelast 30 years, and with several options available, surgeons can utilizewhichever method is most suitable for their patients. There is no one absolutebest method of nipple reconstruction for all patients. Some patients arecomfortable without having a nipple, and do not wish to have further surgery.Others choose the non-surgical option of tattooing without reconstruction. Thisallows color pigmentation to simulate the nipple areola without the contour ofan actual nipple. Still, the reconstruction of the nipple areola helps to putthe finishing touches on the new breast after a long journey in reconstruction.
Afteroptimal symmetry between the breasts has been achieved, the nipple areolareconstruction can be done. There are a number of factors that help determinewhich method of nipple reconstruction is right for you. These include the qualityof tissue on the reconstructed breast, and whether you are having nipplereconstruction with or without a surrounding graft. Even more important, isyour surgeon’s preference.
Historically,one technique included sharing a piece of the nipple from the opposite breast.This surgery is not used today, because it transfers breast tissue to thereconstruction that could potentially form a new cancer. Another method used inthe past involved taking a full thickness skin graft from the labia to create adark colored areola. This outdated technique leaves a scar in an undesirablelocation. Also, these grafts may be hair bearing, and areolar pigment is easierachieved with medical tattooing.
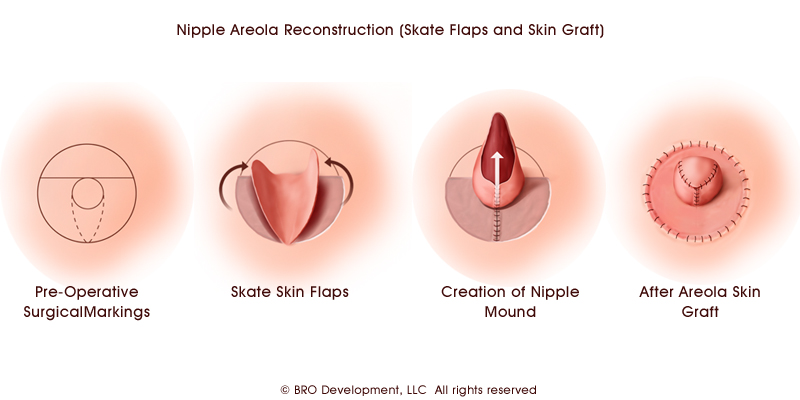
Inmodern approaches to nipple reconstruction, the nipple mound is created fromskin taken as a local flap on the reconstructed breast. Various local flapshave been described, including the Skate flap, the C-V flap and the Star flap.Regardless of which approach your surgeon chooses, the outcome will be a nipplemound. The areola can then be either tattooed, or it can be reconstructed witha skin graft taken from elsewhere on the body. Common donor sites for the graftinclude the abdominal scar from a flap reconstruction, the inner thigh, or thebuttock crease.
|
Nipple Areola Reconstruction (Skate Flaps and Skin Graft)
Click Image to Enlarge
|
Allnipple reconstructions lose some projection over time as part of the normalwound healing process. The risk of wound complications in nipple reconstructionis very low in patients with no history of prior radiation, but common in theradiated breast. In the case of failed nipple reconstruction, it may benecessary to revise the reconstruction with another local skin flap. Sometimes,the use of dermis or fat grafts, and fillers such as Radiesse, may be necessaryto improve nipple projection. AlloDerm® has also beenutilized by some surgeons at the time of nipple reconstruction to maximizeprojection and correct flattening.
Nipplereconstruction is done as an outpatient, ambulatory procedure. The rate ofrecovery depends on what other revisions are done simultaneously, and where thedonor site for the areola graft is located. Once you have healed, you will havethe tattooing done in your surgeon’s office. Refer to the Nipple AreolaTattoosection for details on this procedure. Also you may refer to the Post-OperativeNipple Reconstructionsection to learn about care after nipple surgery.
|
Photos and Doctor Commentary
|
|
|
This patient underwent bilateral mastectomies and TRAM flap reconstruction. Her nipple reconstruction was completed with skate skin flaps. Each areola is a skin graft taken from the healed TRAM flap scar on the abdomen. This is the final appearance after nipple areola tattoo.
|
Nipple areola reconstruction after bilateral TRAM flaps
|
|
|
|
|
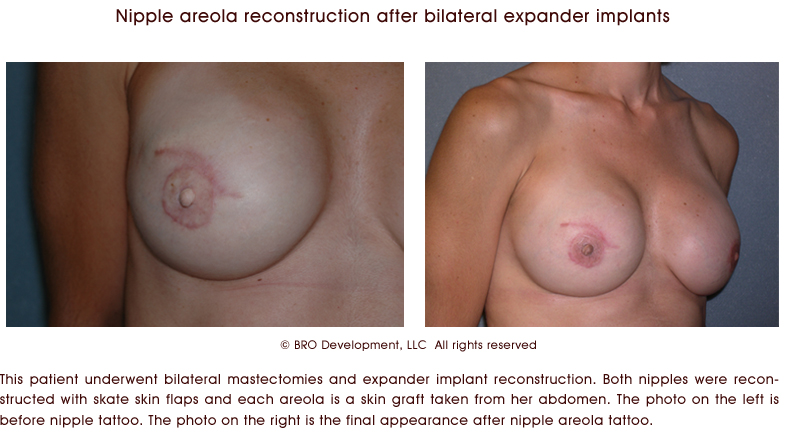
Nipple areola reconstruction after bilateral expander implants
Click Image to Enlarge
|
This patient underwent bilateral mastectomies and expander implant reconstruction. Both nipples were reconstructed with skate skin flaps and each areola is a skin graft taken from her abdomen. The photo on the left is before nipple tattoo. The photo on the right is the final appearance after nipple areola tattoo.
|
Nipple Areola Tattoo
The finishing touch to breast reconstruction is having your nipple areola tattooed. This is usually done in your plastic surgeon’s office. Tattooing is a simple, fast procedure. There is no need to be scared. If you are matching a new nipple areola to the existing breast, your plastic surgeon will mix various colors and shades to get the correct pigment. If you had bilateral reconstructions, your surgeon can use your preoperative photos to recreate the nipple color, or you can pick a new color that you like against your skin tones. As with any tattoo, the pigment will fade in time. Getting the right shade of color may require more than one tattoo procedure. If you are having nipple tattooing alone, with no nipple reconstruction, you may want to look for a doctor that specializes in giving your tattoo a three dimensional appearance.
If you have had a breast implant and regained some breast skin sensation, your plastic surgeon may need to give you an injection of local anesthetic. Most patients with flap reconstruction have little sensation. After drawing the outline of the areola, the surgeon will place the tattooing instrument against your breast. You may feel a pushing and vibrating sensation, as many small needles transfer pigment into your skin. The entire process can take as little as fifteen minutes.
|
Photos and Doctor Commentary
|
|
Nipple areola tattoo procedure
|
Immediately after nipple areola tattoo procedure
|
Click Image to Enlarge
|
The nipple tattooing process, completed as an office procedure, is shown here. Immediately after the tattooing is completed, the colors are difficult to see because the pigment mixes with the blood.
Final appearance after the tattooing has healed
Click Image to Enlarge
|
|
|
|
|
|
|
Allograft Use in Breast Reconstructive Surgery
|
Description
Acellular tissue matrix is a specially-prepared tissuereplacement product that is created from native human skin that has beenprocessed so that the basement membrane and cellular matrix remain intact.However, the processing removes cellular components that can lead to bothrejection and infection.
Reports of use of this tissue matrix (allograft) in breast reconstructivesurgery are being published. Most reports describe use of the allograft tocreate a “hammock” or “sling” to provide improved inferior and lateral supportfor breast implants. This has been used in immediate and delayed reconstructionas well as in revision of prior reconstructive surgery. There also is someinterest in using the allograft in nipple reconstruction post-mastectomy.
The potential advantages of using this device are to reduce the total time forreconstructive surgery post-mastectomy, minimize the likelihood of implantmigration, and improve esthetic outcomes. For example, use of the allograft mayallow for implantation of a silicone implant during immediate reconstruction insome patients.
AlloDerm is an acellular dermal matrix (allograft) derived from donated humanskin tissue supplied by US AATB-compliant tissue banks utilizing the standardsof the American Association of Tissue Banks (AATB) and U.S. Food and DrugAdministration’s (FDA) guidelines. Since AlloDerm is regarded as minimallyprocessed and not significantly changed in structure from the natural material,the FDA has classified it as banked human tissue.
Note: This policy only addresses use of the allograft material for use inbreast reconstructive surgery.
Policy
Use of allograft material may be considered medically necessaryfor use in breast reconstructive surgery:
- when there is insufficient tissue expander or implant covereage by the pectoralis major muscle and additional coverage is required,
- when there is viable but compromised or thin post-mastectomy skin flaps that are at risk of dehiscence or necrosis, or
- the infra-mammary fold and lateral mammary folds have been undermined during mastectomy and re-establishment of these landmarks is needed.
Post-Operative Tattoo
You will have ointment and a gauze dressing placed inside yourbra or taped onto your breast reconstruction. You will need gauze andBacitracin or Aquaphor at home in order to change the dressing every few hoursfor the first few days.. It is best to use a non-adherent type of gauze dressingand a generous amount of ointment on the tattoo. For the first day, the tattoowill bleed or ooze a mixture of ink and blood. The color of the tattoo willappear to be quite dark. Do not panic, this is completely normal. You will needto care for the tattoo for several days. During this period, the ink and bloodwill scab off, and the true color of the tattoo will be revealed. It isimportant not to let the tattoo get dry. While in the comfort of you own home,if you can sit without clothing and maintain the ointment over the tattoo, thehealing process will be faster. Having clothes rub against the tattoo may beuncomfortable, and the ink or scabs may stain your clothing.
The tattoo will mature over the course of several weeks. If youfind the color is too light, you can always go back and have more pigmentadded. If you already had an emotional boost from having your nipple surgery,once the tattoo has healed, you are officially done!
Post-Operative Abdominal Flap
If you have not yet had your surgery, you may want to begin byreading the Preparing for Surgery section for TRAM flapand other abdominal flap reconstruction. If you have taken the time to preparefor surgery, all that will be left to do is rest and heal. In this section youwill find tips to help you recover, and learn about how surgery might affectyou. It is important to remember that everyone is different, and we all heal atour own pace. What works for some, may not work for others. We hope thissection will serve as a helpful guide for you.
In the Hospital
Upon waking up from surgery, you may be confused as you awakenfrom anesthesia. Others may feel sharp and alert as soon as their breathingtube is removed. If you have never had surgery with a breathing tube, it isimportant to remember not to fight it when the doctor takes it out, and take anice deep breath once it is removed. Your throat may feel raw and you may havetrouble speaking at first, but this will wear off soon. If you feel any nausea,do not be afraid. You will be surrounded by a team of doctors and nurses thatwill take care of you, no matter what may arise.
Once in the recovery room, you will have strong painmedication, and you will probably sleep a lot. You will have compressionsleeves on your legs that help with circulation. You will also be given anincentive spirometer, which is a breathing device that helps you expand yourlungs. Nurses will check on you often, especially if you have had microsurgery,to make sure the blood supply to the flap is not compromised. You will probablybe visited by a pain management specialist to help make you as comfortable aspossible. A computerized pain medicine pump may be attached to your IV thatallows you to receive pain medicine at the touch of a button. The drains willusually be secured together to make it easier to monitor your drain outputs.Most patients will have two drains for each reconstructed breast and two drainsin the abdomen. The nurses will care for your drains, and during that time youwill learn how to care for them yourself.
The day after surgery, you will be helped out of bed into achair. A catheter in the bladder from the operation will drain continue todrain urine so you will not have to go to the bathroom by yourself yet. Thiscatheter will be removed when you are more comfortable and mobile, usually bythe second or third day after surgery. You will have more pain in the abdomenthan in the breasts. If you are having a sentinel lymph node biopsy, or othernodes removed, you may feel sore, especially if the drains exit from under yourarms. Most of the breast area will feel numb. You will be slightly hunchedover, and you may have feelings of tightness and discomfort in your abdominalarea. Getting in and out of bed is usually the hardest part in the beginning.You won’t have the benefit of a hospital bed once you get home, so it’s helpfulto have someone give you support. From a reclining position, with your feet asclose to the floor as possible, your caretaker should place their right hand onyour lower back, and hold your left arm or hand in their left hand. On thecount of three, you want to get up, using their hand on your back for a littlepush. If you try this, and do it too slowly, you will feel pulling on yourabdomen. After a few tries you will find what works best for you. You have towill yourself to get up, and walk in the hall, or in your hospital room. Thesooner you can do this, the sooner you can get out of the hospital. Many peoplethink they should stay in the hospital longer, but this is unnecessary. Youwill heal and rest much more comfortably in your own home.
Recovery at Home
Upon discharge from the hospital, your nurses and doctor willgo over what you need to do at home. You will be given a prescription for painmedication, and an antibiotic. Please refer to Preparing for Surgery for tips about thecar, and what to wear home. When you get home you will need plenty of rest. Besure to stay hydrated. The sooner you can stop taking the narcotic pain pillsand switch to Tylenol, the easier your recovery will be. Some women have aneasier time in the beginning than others. You may be too tired to shower duringthe first week, but if your surgeon gives you permission, and you feel up toit, you can shower with the help of a caregiver. If you have a deep tub, youmay have problems climbing over it. You will need to pin all of your drainseither to a Velcro drain belt, or you may be given something in the hospitallike a gauze necklace to support the drains around your neck. It may help ifyou have a shower stool (you can get them in most drug stores) so you can sitdown in the shower, and someone can help you wash. Alternatively, you may buy(or obtain from the hospital) packs of disposable wash cloths. As the drainscome out, it will be much easier to shower.
You will most likely see your surgeon weekly until the lastdrain has been removed. You cannot rush removing the drains; as bothersome asthey may be, they are essential to proper wound healing. Generally once anindividual drain produces less than 20 to 30 cc’s in a 24 hour period, yoursurgeon will remove it. In most patients, the drain removal does not hurt.
Resuming Activity
During this time, it is important that every day, little bylittle, you start to stand up straight. By the third week, you should no longerbe hunched over. Do not be afraid to stand up straight; it is normal to feeltightness in your abdomen. The sooner you are standing up straight, the sooneryou will be able to admire your new breasts in the mirror. Flap breasts mayfeel hard at first, but with every week that passes, the swelling will subside,and the breast will get softer and softer. Early after surgery, you do not needa bra, but if you feel you need something, many women recommend shelf bracamisoles, that are soft. You don’t want anything that compresses thereconstructed breast too tightly, and you don’t want underwire bras that mayirritate your healing scar. You will notice changes in the breasts especiallyover the first eight weeks. Keep in mind that during the second surgery, yoursurgeon will address any areas of aesthetic concerns you may have.
The abdominal discomfort you experience should begin to subsideonce the drains are removed. Sleeping will become more comfortable, however, itmay take time before you are able to sleep on you stomach. Some women find thatgetting a prescription from their surgeon to attend physical therapy helps themget back into normal activities more quickly. It is important to find aphysical therapist that has experience with breast cancer patients. You do notwant a physical therapist that deals only with sports injuries.
Within four to eight weeks you should be back to most of yournormal activities. You will still have some tightness in your abdomen. This iscompletely normal and can last for a few months. It is important to listen toyour body. While you may feel fine driving and doing household chores, it mayrequire a little more time before getting back to advanced Yoga or Pilatesclasses.
Intimacy
Many women have asked when it is okay to resume sexualactivity. Physically, it is safe once your drains are removed, and you feel upto it. Emotionally, it will take as much time as you need. Some women feeluneasy about not having nipples. If this is the case, wearing a camisole maymake you more comfortable. The general concern is wondering how your partnerwill feel. If you are comfortable and confident with the process ofreconstruction, you can ease any concerns your partner may have. The mostcommon concern partners may have, is that they will hurt you if they touch youthe wrong way. It is helpful to communicate, and be receptive to what yourpartner is saying. If you find yourself having a hard time emotionally, it maybe helpful to talk with other women who have already had reconstruction, or toseek help from a counselor.
The important thing to remember is that every day is betterthan the one before. The pain you feel in the hospital will soon become adistant memory. The scars will fade over time, and once you have completed thefinal stages of reconstruction, you will regain a sense of wholeness that willtruly help you to move beyond cancer.
Print Page